Novel bispecific antibodies – Part 2 – immunology, asthma and atopic dermatitis
In 1986 - nearly 40 years ago - the first antibody therapy was FDA-approved: muromonab-CD3 (Orthoclone OKT3®), a murine monoclonal antibody targeting human CD3 expressed on T cells. This therapy was used to treat steroid refractory organ transplant rejection, a very serious inflammatory condition. The first biologic therapy targeting tumor necrosis factor (TNF) was infliximab (Remicade®), which was approved by FDA in 1998. Remicade was the first TNF inhibitor to be widely used in clinical practice, setting off a stampede of drug development targeting cytokines, small proteins secreted by immune cells and many other cell types. Cytokines regulate many cell activities including immune responses, inflammation, cell growth and proliferation and so on. Cytokines can be roughly grouped into a few key classes:
Interleukins (ILs): Cytokines that mediate communication between immune cells and between immune cells and the broader cellular environment.
TNF and TNF-related proteins: Pro-inflammatory cytokines involved in immune cell activation, proliferation and differentiation.
Interferons (IFNs): Cytokines that stimulate anti-viral immunity and directly inhibit viral replication.
Chemokines: Cytokines that attract immune cells to specific sites of inflammation.
Growth Factors: Cytokines that promote cell growth and differentiation.
Biologic therapies targeting cytokines treat numerous inflammatory and autoimmune diseases by blocking these activities. Examples include:

The list goes on and on. This is a highly successful class of therapeutics, and novel targets and novel biologic designs are being pursued by innumerable companies and labs. Our goal today is to look at a few of the bispecific antibodies in development for asthma and atopic dermatitis and consider their chances in an ever-more competitive therapeutic landscape.
Drug development in this bispecific space is a question of mixing and matching targets and aligning the resulting drugs with particular indications. Some of the mixing and matching is straightforward, for example, you can infer from the table that pathways that regulate atopic and asthmatic diseases – IL-4, IL-5, IL-13, TSLP (among others) – might pair nicely in bispecific format. If we focus on TSLP bispecifics we can quickly get a sense of the landscape:
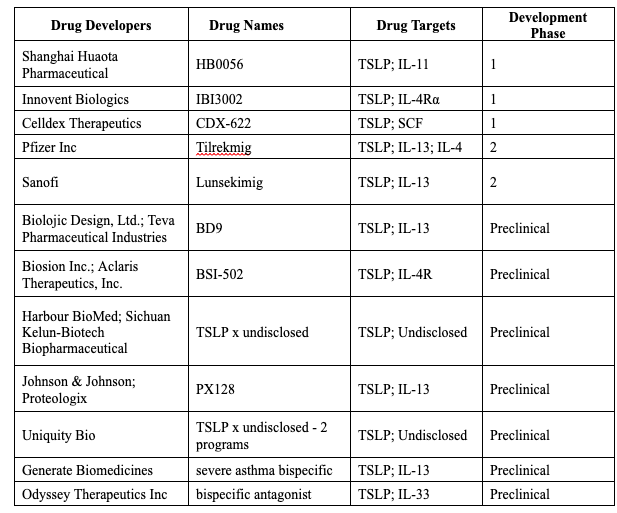
Recall we are leaving out TSLP-targeting antibody programs, of which there are many. We want to jump here to the next wave which are the bispecific programs. We think a few notable themes are evident:
There are only 5 programs in the clinic, dominated by the 2 pharma heavy weights Sanofi and Pfizer. Sanofi certainly makes sense, as their IL-4/IL-13 receptor antibody drug dupilumab (Dupixent®) is an asthma blockbuster just now breaking into COPD. Looking at the sales trajectory we can see why this is such an attractive marketplace.

Pfizer’s positioning also makes sense as their approved targeted drug for atopic diseases is an oral JAK inhibitor (abrocitinib). JAKs signal downstream of the cell surface receptors for cytokines so there is a biology connection. The issue is more specificity as JAKs signal downstream of many different receptors and therefore the toxicities associated with JAK inhibition can be severe. Moving into the very specific biologics space with bispecifics may provide enhanced efficacy with less tox. They appear to have dived deeply into this space (see below).
Uniquity Bio is like a spec-house: built by a financer (Blackstone Life Sciences) who put in $300M with a triple-play on TSLP: first, a straight monoclonal antibody program, and then 2 undisclosed bispecific programs. This type of targeted investment is a clear sign that this is a space to watch.
Most of the programs we find are pretty safe TSLP x IL-4 and/or IL-13 bispecifics, but there are three unique programs in the table, targeting TSLP + IL-11, TSLP + SCF and a third program, quite novel I think, targeting TSLP + IL-33, from Odyssey Therapeutics. Odyssey is another spec-house type of company, heavily backed by big venture names OrbiMed and SR One. This is a smart shop led by former chemist and immunologist Gary Glick and packed with absolutely top-tier scientific advisors: (https://odysseytx.com/leadership/?category=scientific-advisory-board).
Let’s go back just for a second to Pfizer and their pipeline of new programs in immune diseases. It’s hard to tell exactly what these therapeutics actually are, and it’s puzzling that some are just labeled new molecular entities, which is vague, but they certainly are in the space now in a big way.

And they are building dual antagonists IL-4/IL-13 + TSLP and IL-4/IL-13 + IL-33.
But back to our table - what is driving all of this bubbling TSLP x IL-13 drug development?
Data from Sanofi, the current market leader driving IL-4/IL-13 receptor antibody drug Dupixent® and data from Amgen and AstraZeneca, the developers of tezepelumab (Tezpire®), the up-and-coming anti-TSLP therapeutic.
Sanofi’s SAR443765 (aka lunsekimig) is a bispecific NANOBODY® molecule. We love using nanobodies at Aleta Bio and they are present in all of our CAR T Engager and T Cell Engager programs. Nanobody refers to a class of antibodies that are generated in camelids, i.e. llamas, alpacas and camels. These are very small and very stable proteins that can be woven together to make multi-targeting therapeutics. Sanofi acquired this technology via its purchase of Ablynx. In the lunsekimig program, this technology is put to good use.
How cool is this protein?

Not only are there two antibody binders for both IL-13 and for TSLP, they actually bind to different epitopes on those target proteins - so called biparatopic binding that enhances binding affinity for the target (‘epitope’ refers to the part of a protein that is bound by the antibody domain, ‘paratope’ refers to the part of the antibody that binds the protein). Plus, the anti-albumin binder targets serum albumin, an abundant protein in the bloodstream that confers a long circulating half-life on proteins that it binds. Thus, anti-albumin binds to albumin and the entire therapeutic gains long half-life in circulation.
In a Phase 2 clinical trial in moderate to severe asthma, a single dose of lunsekimig resulted in a significant reduction in FeNO compared to placebo at week 4. The FENO (fractional exhaled nitric oxide) test measures the amount of nitric oxide in the breath and is a non-invasive way to assess airway inflammation. The comparison of efficacy of lunsekimig to both anti-TSLP and anti-IL-13 therapeutics is shown below in this figure from a Sanofi presentation:

The point they are making is very clear - the bispecific therapeutic dramatically outperforms the single target antibodies across these clinical trial results. Our conclusion - bispecific therapeutics are poised to make a dramatic difference in severe asthma, and the interest in this class in intense for good reason.
Next time we’re going to look at bispecifics that work on a different set of immunology indications. It’s a space where some very unusual therapeutics are being developed and in this makes it quite interesting.
Stay tuned.